Investors
Corporate Overview
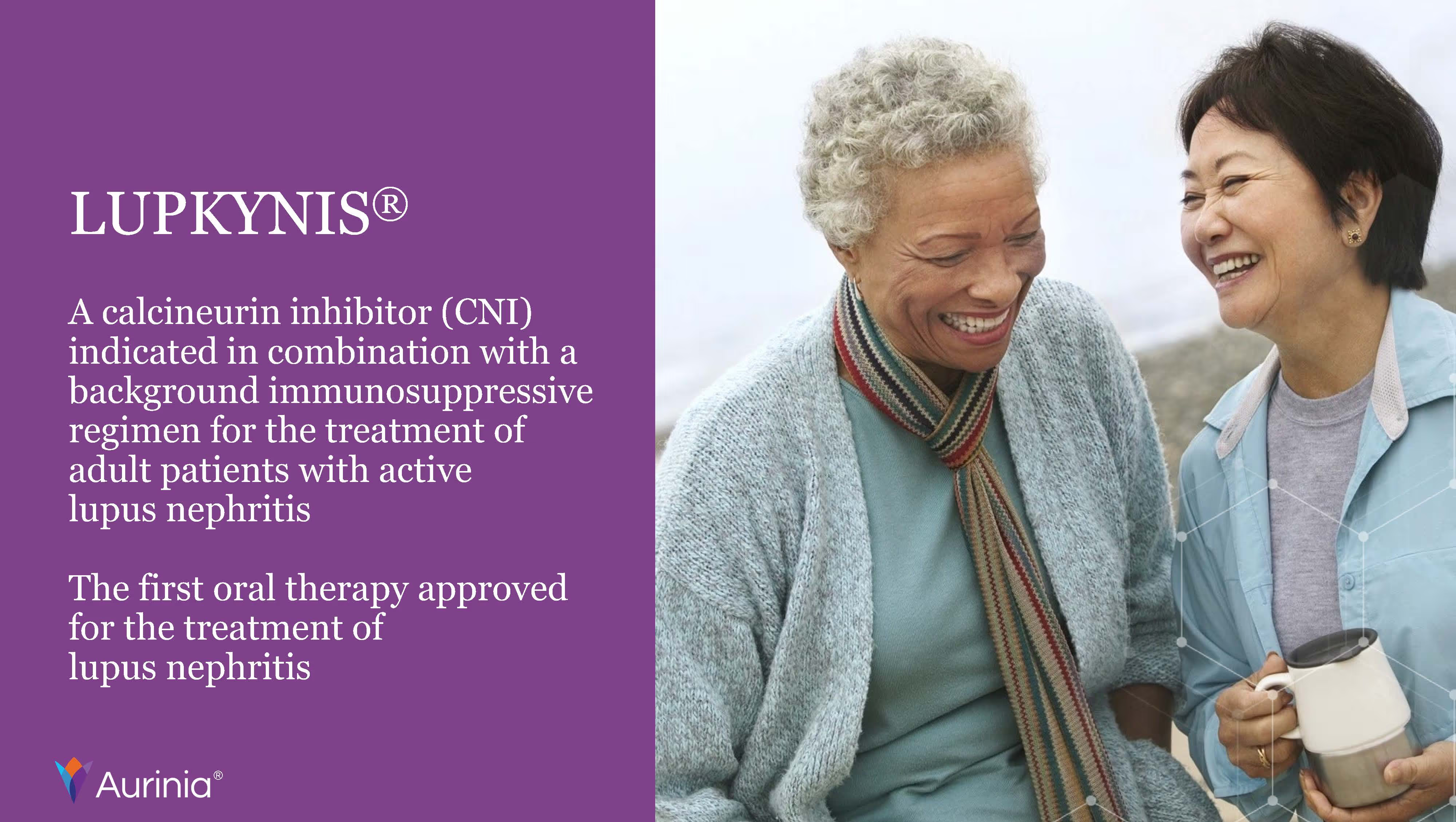
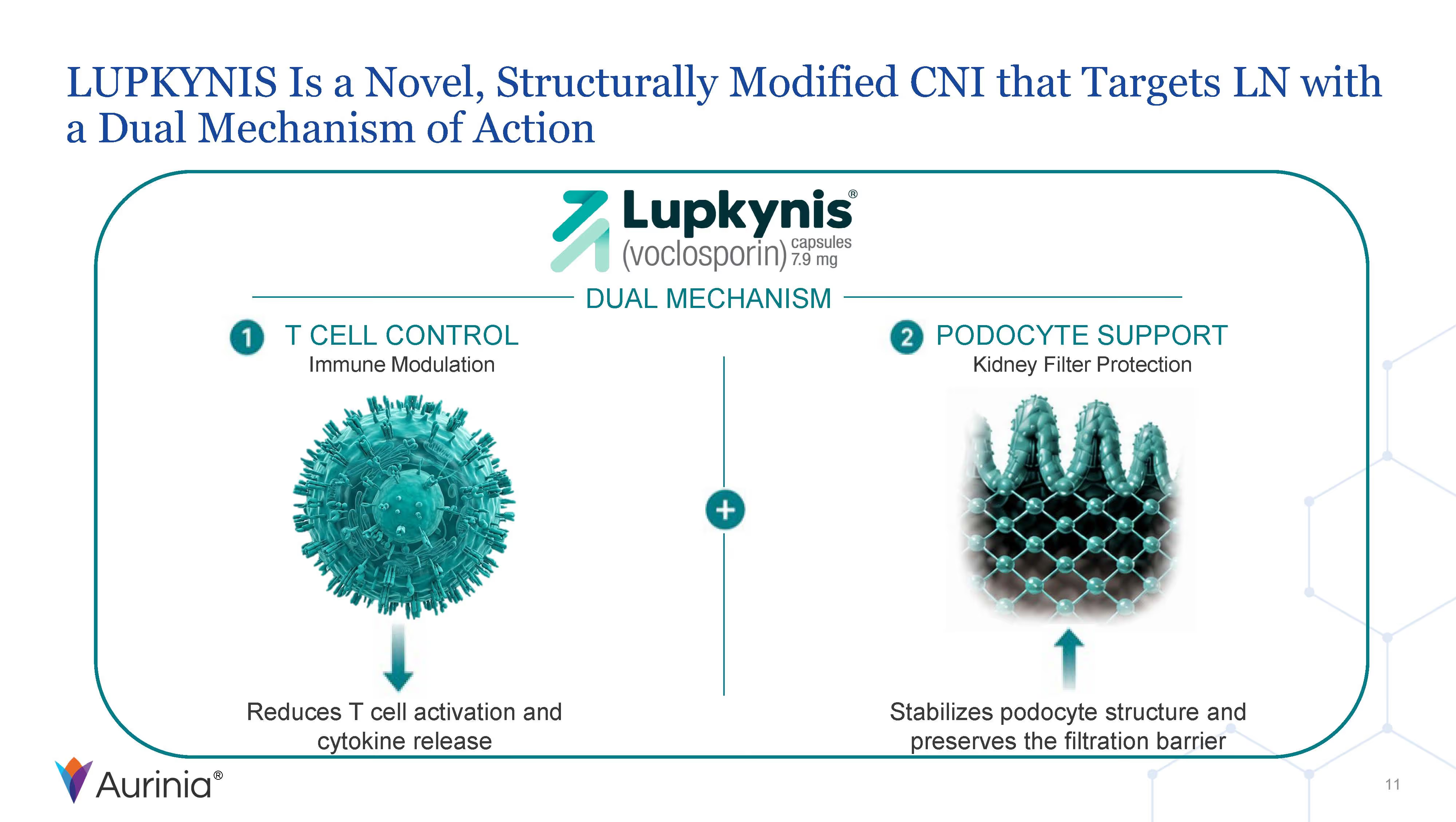
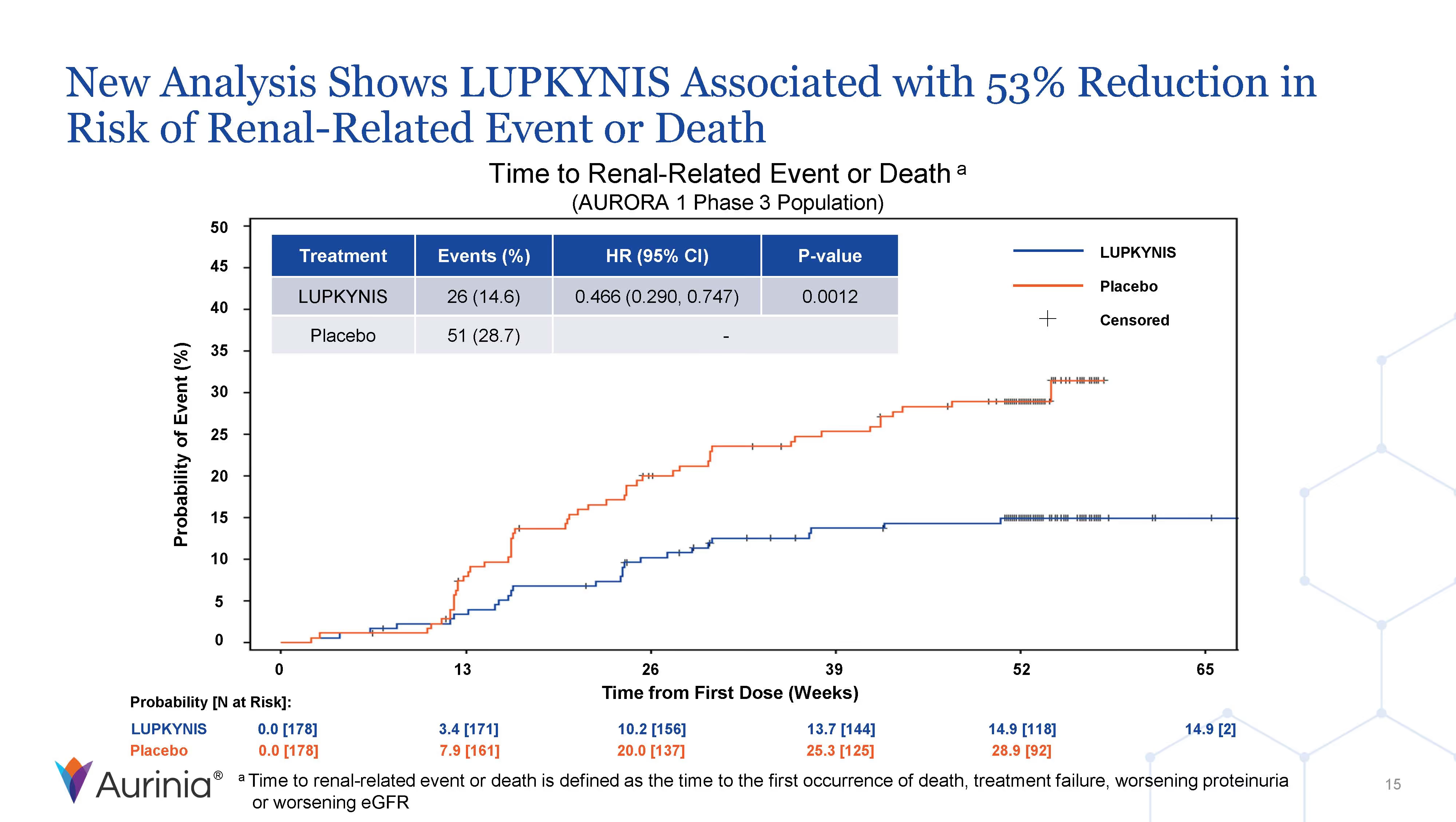
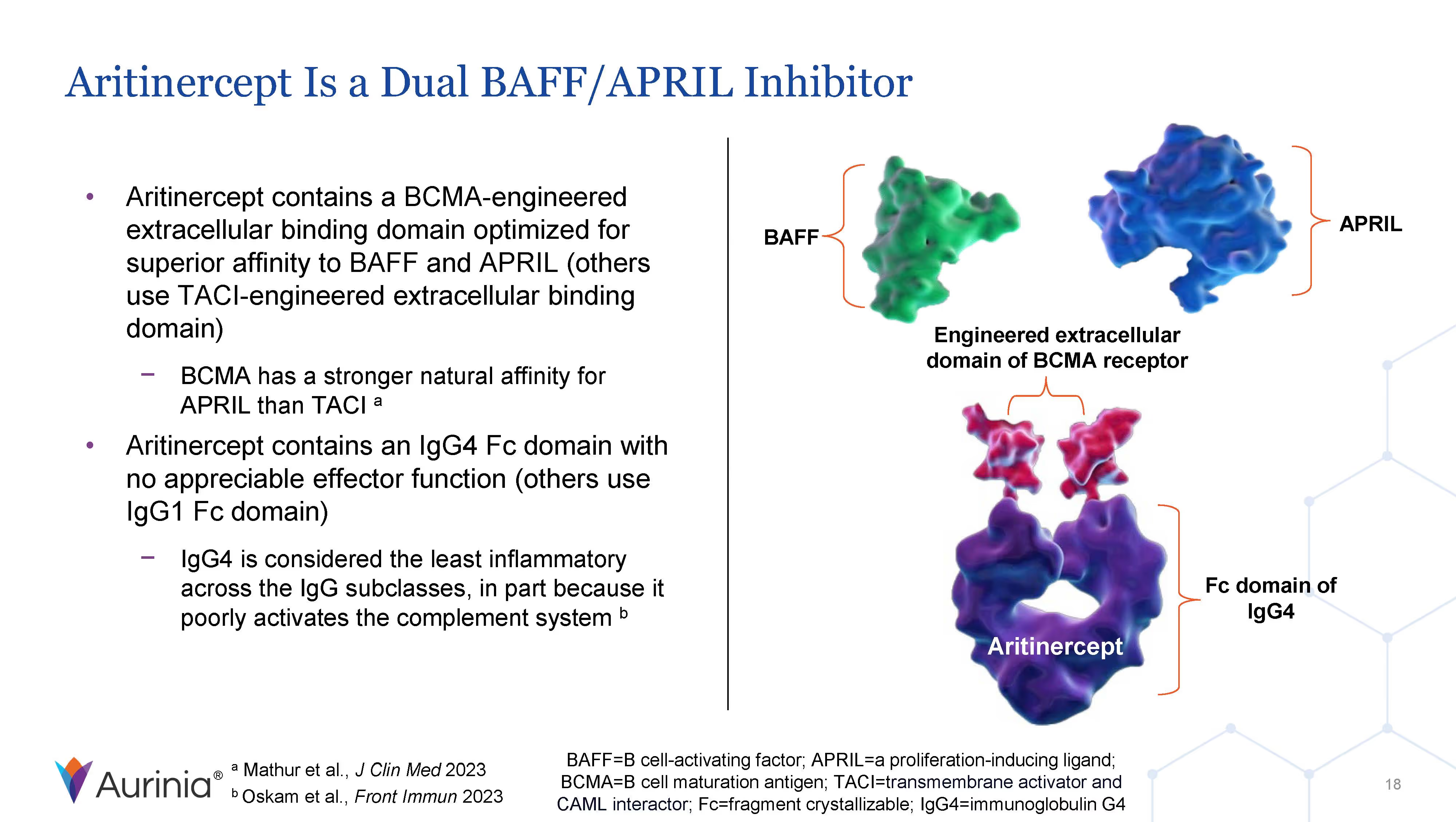
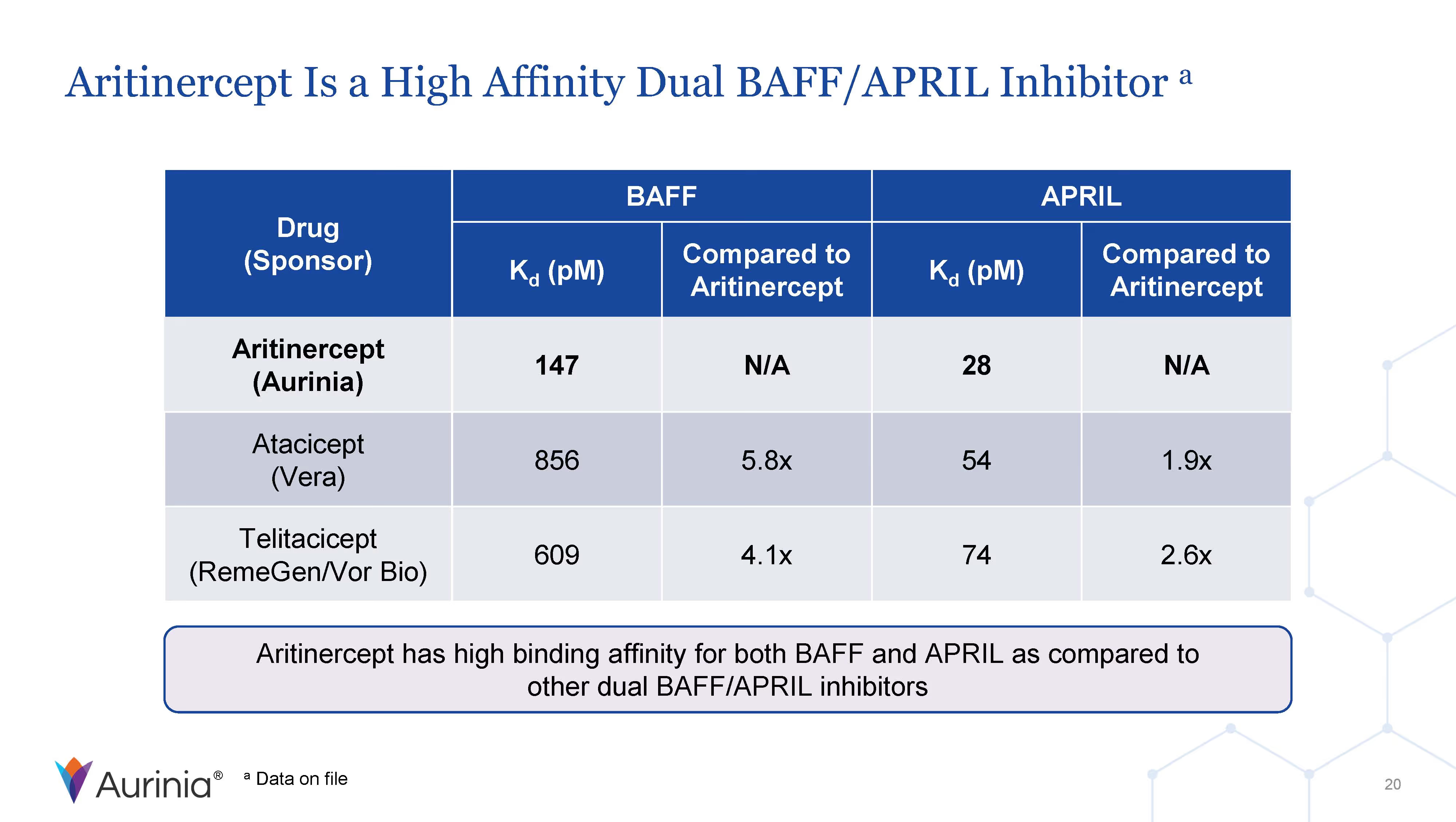
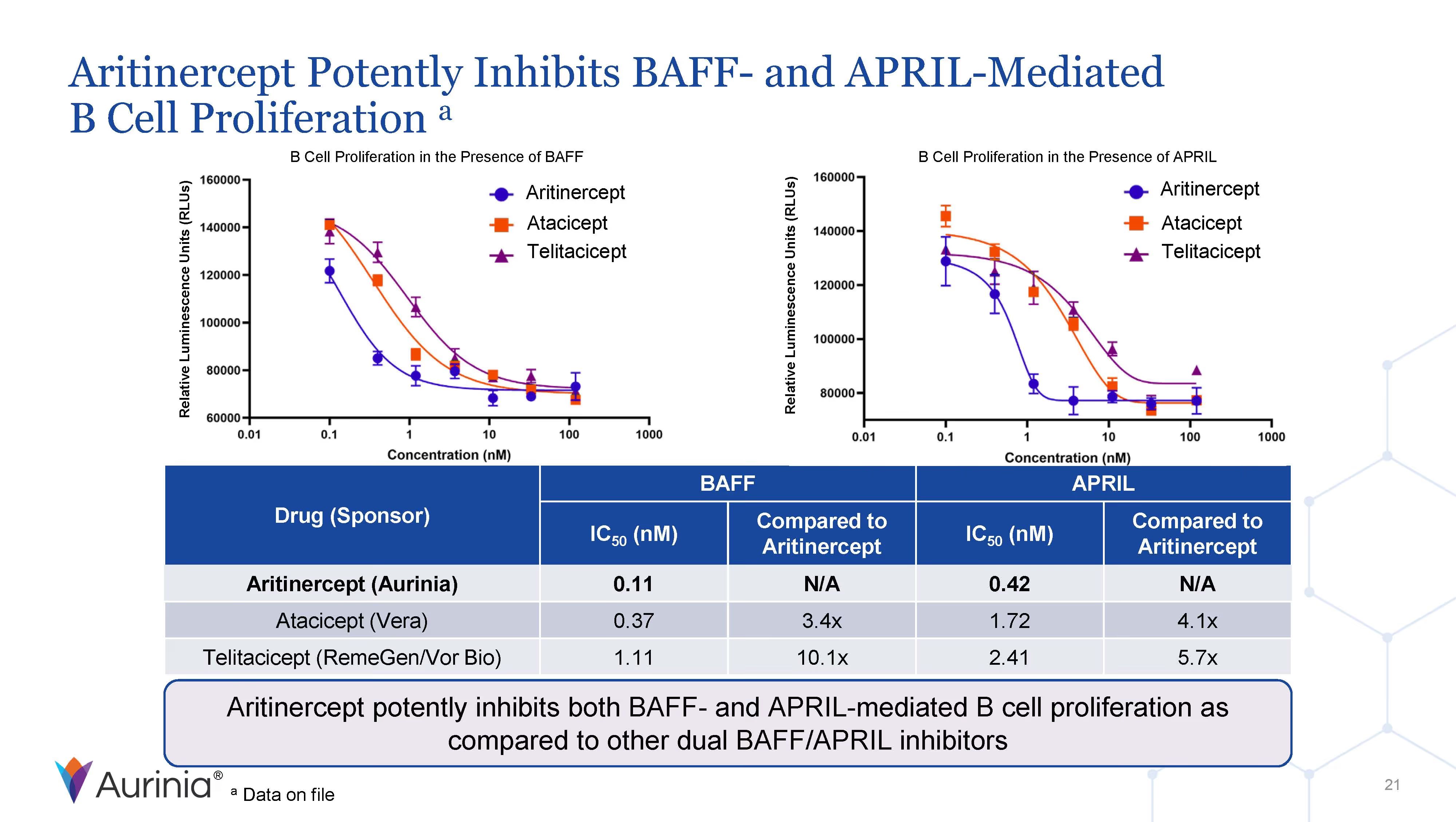
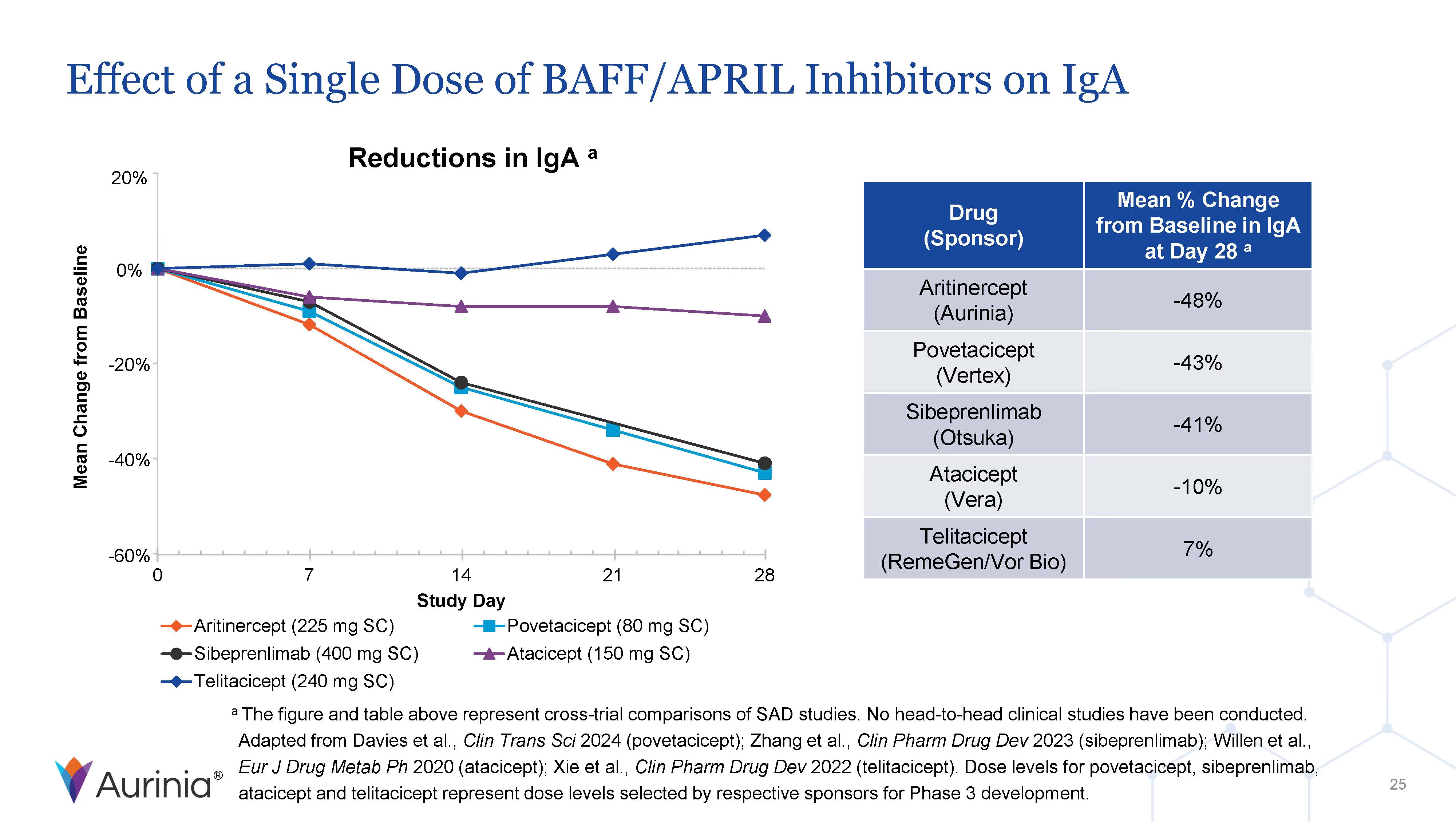
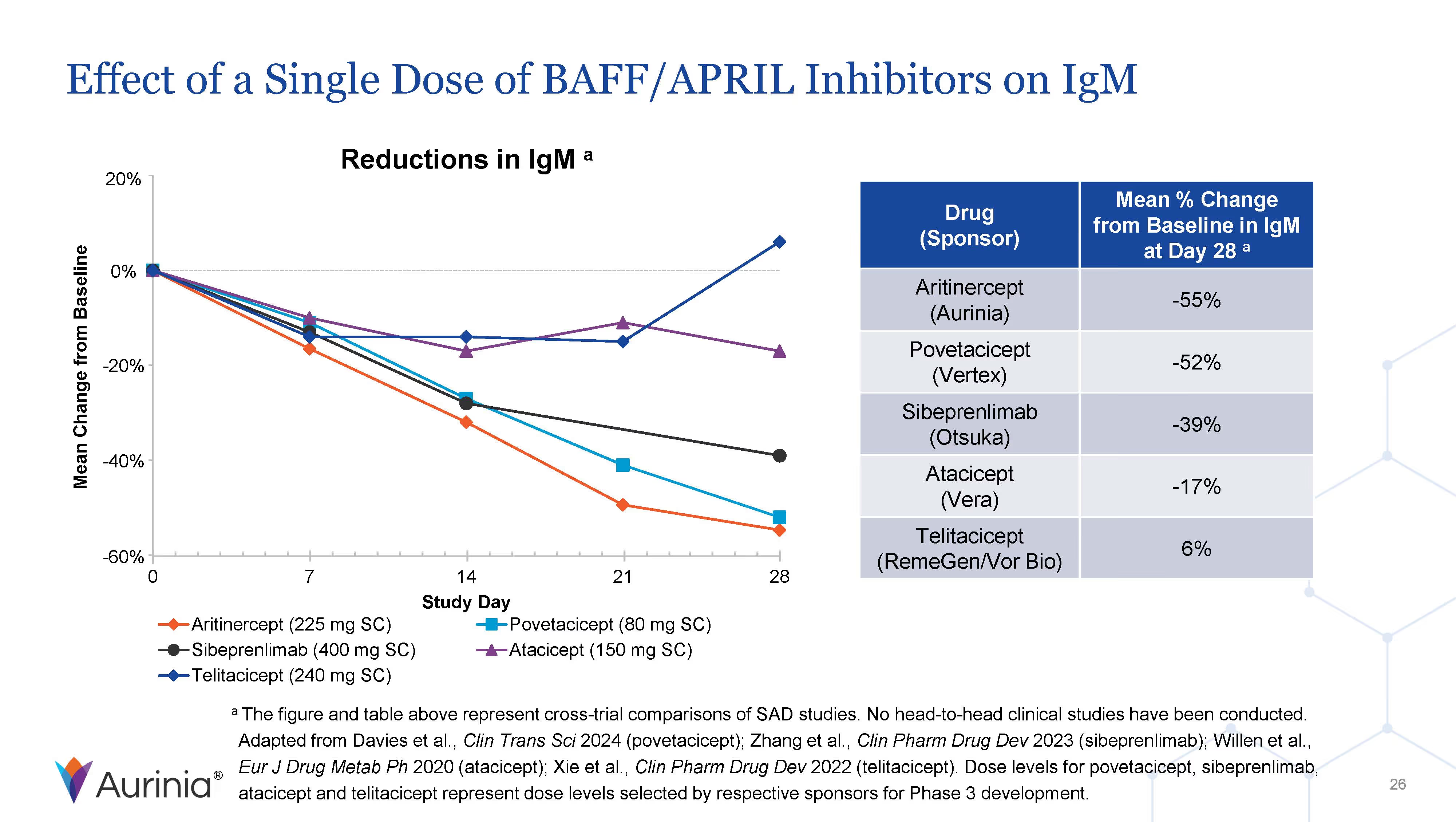
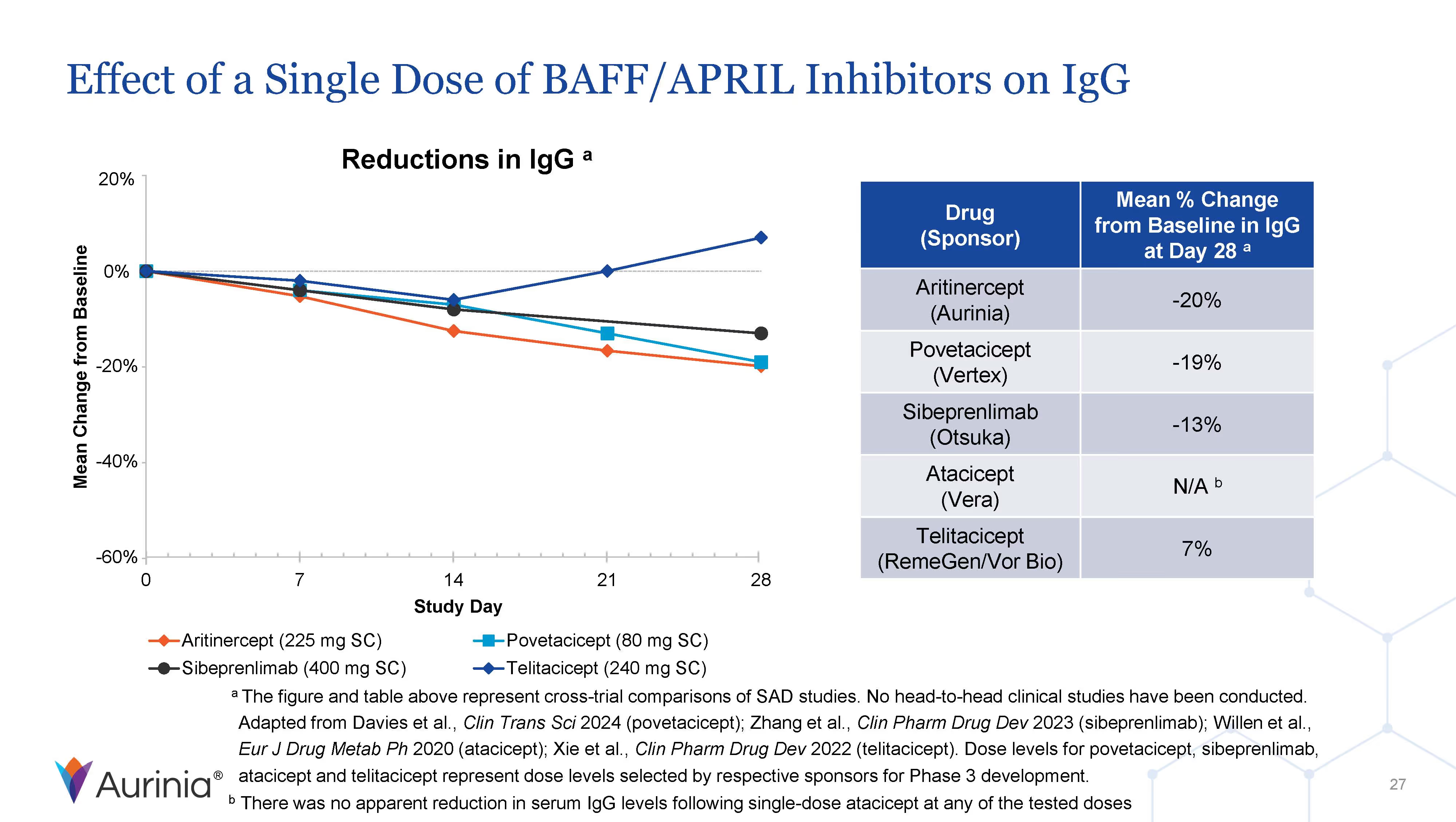
Aurinia Pharmaceuticals Inc. is a biopharmaceutical company focused on delivering therapies to people living with autoimmune diseases with high unmet medical needs. In January 2021, the Company introduced LUPKYNIS (voclosporin), the first FDA-approved oral therapy for the treatment of adult patients with active lupus nephritis. Aurinia is also developing aritinercept, a dual inhibitor of B cell-activating factor (BAFF) and a proliferation-inducing ligand (APRIL) for the potential treatment of autoimmune diseases.









Email Alerts
Stock Information
NASDAQ Global Market: AUPH
$16.46
+0.32
/
+1.98%
1.17M
Volume
Last update:
Closed at 06/18/2026 4:00PM ET
Pricing delayed by 15 minutes
Upcoming Events
There are no upcoming events scheduled at this time.
Past Events
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.
Nov 7
-
Nov 7, 2024
Nov 7, 2024 8:30 PM
EDT
2024
Third Quarter 2024 Financial Results Conference Call
Oct 23
-
Oct 27, 2024
Oct 23, 2024 12:00 AM
2024
American Society of Nephrology (ASN) Kidney Week 2024
Sep 17
-
Sep 17, 2024
Sep 17, 2024 3:05 PM
EDT
2024
2024 Cantor Fitzgerald Global Healthcare Conference
Sep 10
-
Sep 10, 2024
Sep 10, 2024 10:30 AM
EDT
2024
H.C. Wainwright 26th Annual Global Investment Conference
Aug 1
-
Aug 1, 2024
Aug 1, 2024 8:30 AM
EDT
2024
Second Quarter 2024 Financial Results Conference Call
No Results Found
Please try different keywords or filters.
SEC Filings
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.
Date
Filing Type
Description
Download
Date
June 8, 2026
2026
Filing Type
4Description
Statement of Changes in Beneficial Ownership
Section 16 Filings
Date
June 8, 2026
2026
Filing Type
4Description
Statement of Changes in Beneficial Ownership
Section 16 Filings
Date
June 8, 2026
2026
Filing Type
4Description
Statement of Changes in Beneficial Ownership
Section 16 Filings
Date
June 8, 2026
2026
Filing Type
4Description
Statement of Changes in Beneficial Ownership
Section 16 Filings
No Results Found
Please try different keywords or filters.
Governance
Committee Charter Documents
Governance Documents
IR Contact
General inquiries can be sent to ir@auriniapharma.com